Facilitated Communication
SPECIAL THANKS TO OUR PANELISTS AT THE 2023 FABA CONFERENCE:
Facilitated Communication and Other Pseudoscientific and Unsubstantiated Treatments: Guidance for Behavior Analysts
(listed alphabetically)
Definition of Facilitated Communication:
- Facilitated Communication (FC) comprises a group of conceptually and procedurally related techniques in which selection-based communication is simulated in an individual by a second individual who provides direct or indirect physical, gestural, verbal, or other guidance for the item selections.
- Used with permission of Dr. James Todd, Professor of Psychology, Eastern Michigan University (Personal communication with Jack Scott; March 8, 2023)
"Because physical assistance is needed for communication to occur, the question has arisen as to whether the facilitator or the individual who is facilitated is responsible for authoring messages." Howard C. Shane and Kevin Kearns (1994)
Variants of Facilitated Communication (facilitator-dependent techniques):
- Rapid Prompting Method (RPM)
- Spelling to Communicate (S2C)
- Assisted Typing
- Facilitated Communication Training
- Supported Typing
"FC has been thoroughly discredited by the scientific community. Most major health, education, and autism advocacy organizations have opposition statements and strongly urge their members not to use FC. Individuals with disabilities deserve to have access to communication technologies and methods currently available for use that promote independence and allow them to make their voices heard without interference from facilitators." www.facilitatedcommunication.org
Statements of Professional Organizations:
| ASHA (American Speech Language Hearing Association) |
It is the position of the American Speech-Language-Hearing Association (ASHA) that Facilitated Communication (FC) is a discredited technique that should not be used. There is no scientific evidence of the validity of FC, and there is extensive scientific evidence—produced over several decades and across several countries—that messages are authored by the "facilitator" rather than the person with a disability. Furthermore, there is extensive evidence of harms related to the use of FC. Information obtained through the use of FC should not be considered as the communication of the person with a disability.
Complete position paper: https://www.asha.org/policy/ps2018-00352/
|
| American Academy of Child and Adolescent Psychiatry (AACAP) |
“Studies have repeatedly demonstrated that FC is not a scientifically valid technique for individuals with autism or mental retardation. In particular, information obtained via (FC) should not be used to confirm or deny allegations of abuse or to make diagnostic or treatment decisions.” Approved by Council, October 20, 1993. Reviewed June, 2008. To be reviewed June, 2013. |
| American Academy of Pediatrics |
“In the case of FC, there are good scientific data showing it to be ineffective. Moreover, as noted before, the potential for harm does exist, particularly if unsubstantiated allegations of abuse occur using FC. Many families incur substantial expense pursuing these treatments, and spend time and resources that could be used more productively on behavioral and educational interventions.” |
| American Association on Intellectual and Developmental Disabilities (AAIDD) |
On January 9, 2019, The Board of Directors of the American Association on Intellectual and Developmental Disabilities (AAIDD) announced that based on current scientific evidence, it “does not support the use of Facilitated Communication (FC) or the Rapid Prompting Method (RPM) as modes of communication for people with disabilities. In the case of FC, there is no scientific evidence supporting its validity, and there is considerable evidence that the messages are authored by the facilitator rather than by the individual with a disability. In the case of RPM, there is lack of scientific evidence for its validity, and concerns about message authorship similar to those for FC have been raised.” |
| APA |
“The short version of this long story is that study after study showed that facilitated communication didn’t really work. Apparently, the positive results that had generated so much enthusiasm were the results of a subtle process in which well-intended facilitators were answering questions themselves - without any awareness that they were doing so. Based on the findings of carefully controlled studies of facilitated communication, the American Psychological Association issued a resolution in 1994 that there was “no scientifically demonstrated support for its efficacy.” |
| ABAI |
“It is the position of the Association for Behavior Analysis that FC is a discredited technique. Because of the absence of ample, objective, scientific evidence that FC is beneficial and that identifies the specific conditions under which it may be used with benefit, its use is unwarranted and unethical.” |
| Autism Speaks |
Autism Speaks does not support Rapid Prompting Method or Facilitated Communication and shares ASHA’s positions on FC and RPM. |
| International Society for Augmentative and Alternative Communication (ISAAC) |
“In conclusion, given ISAAC’s mission to promote the best possible communication abilities and opportunities for persons with limited or no functional speech, ISAAC does not support FC as a valid form of AAC, a valid means for people to access AAC, or a valid means to communicate important life decisions. The weight of evidence does not support FC and therefore it cannot be recommended for use in clinical practice.” |
1993 Frontline “Prisoners of Silence” (includes facilitators with clients)
2022 Rollins College student giving Valedictorian Speech “Be the Light” (prepared with facilitator dependence and played through text-to-speech computer program
https://youtu.be/8g5aJExZQwg
Pseudoscience, junk science, or unsubstantiated therapy? What other techniques may fall in this category?
- Sensory Integration (brushing, joint compression) therapy
- Audio Integration Therapy
- "Astronaut Training"
- Gluten- and Casein-free diets
- Mega-vitamin therapy
- Hyperbaric chambers
- Dolphin therapy
- Brain Balance
- Zones of Regulation (Social Thinking)
Relevant standards in the BACB Code of Ethics:
- 1.06 Maintaining Competence (behavior analysts need to be able to spot pseudoscience and advocate effectively for science-based approaches)
- 2.01 Providing Effective Treatment
- 2.10 Collaborating with Colleagues
- 2.14 Selecting, Designing, and Implementing Behavior-Change Interventions: Behavior analysts select, design, and implement behavior-change interventions that: (1) are conceptually consistent with behavioral principles; (2) are based on scientific evidence…
2.19 Addressing Conditions Interfering with Service Delivery
- 3.06 Consulting with Other Providers
- 3.12 Advocating for Appropriate Services
- 5.03 Public Statements by Behavior Analysts (see 1.01, 1.02): When providing public statements about their professional activities, or those of others with whom they are affiliated, behavior analysts take reasonable precautions to ensure that the statements are truthful and do not mislead or exaggerate either because of what they state, convey, suggest, or omit; and are based on existing research and a behavioral conceptualization.
5.06 Advertising Nonbehavioral Services (see 1.01, 1.02, 2.01) Behavior analysts do not advertise nonbehavioral services as behavioral services…
- RBT CODE 2.0 Behavior-Technician Services: Services provided under the direction of a BACB-required supervisor that are explicitly based on the principles and procedures of behavior analysis and are designed to change behavior in meaningful ways.
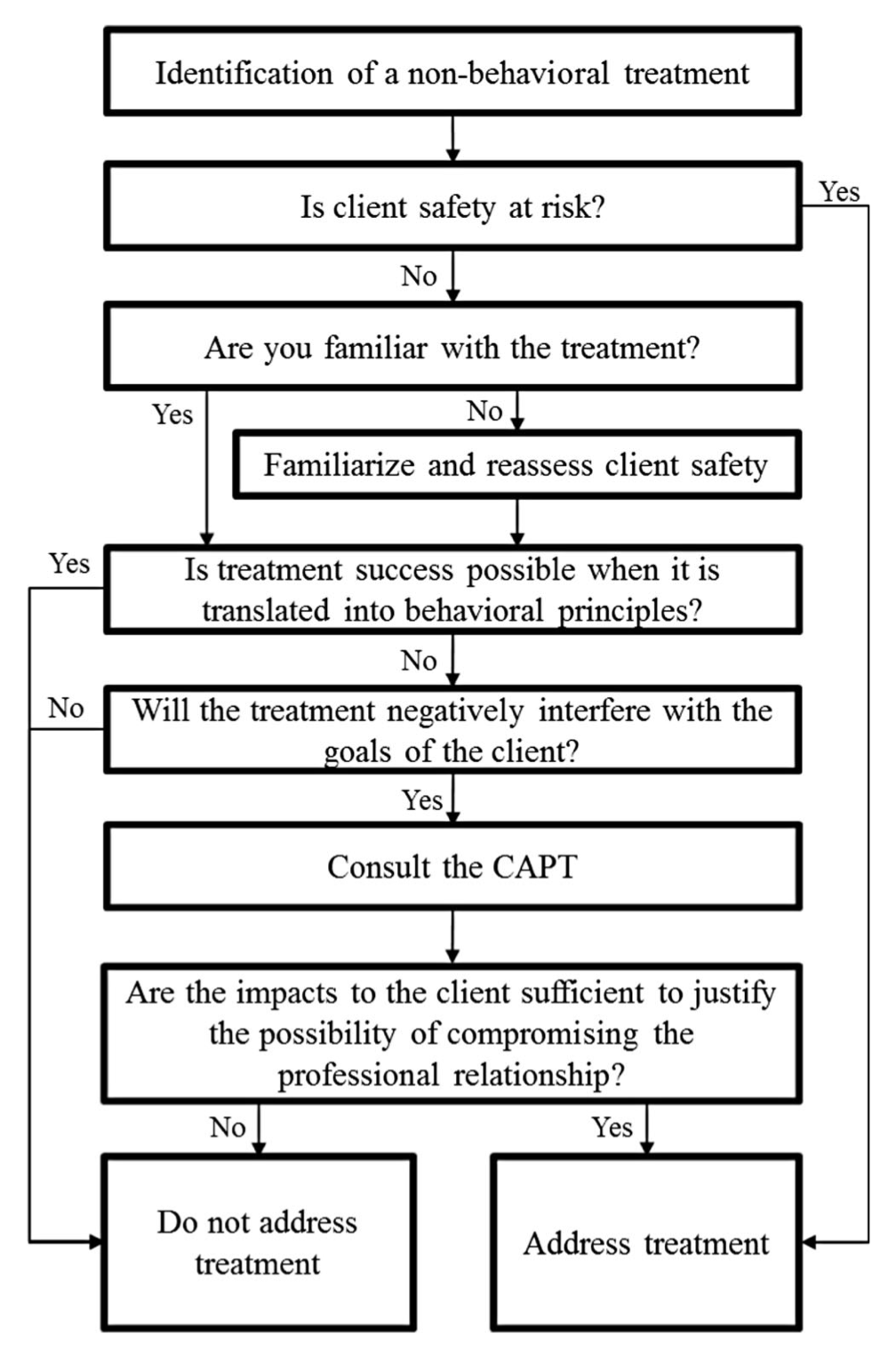
Brodhead's Flowchart:
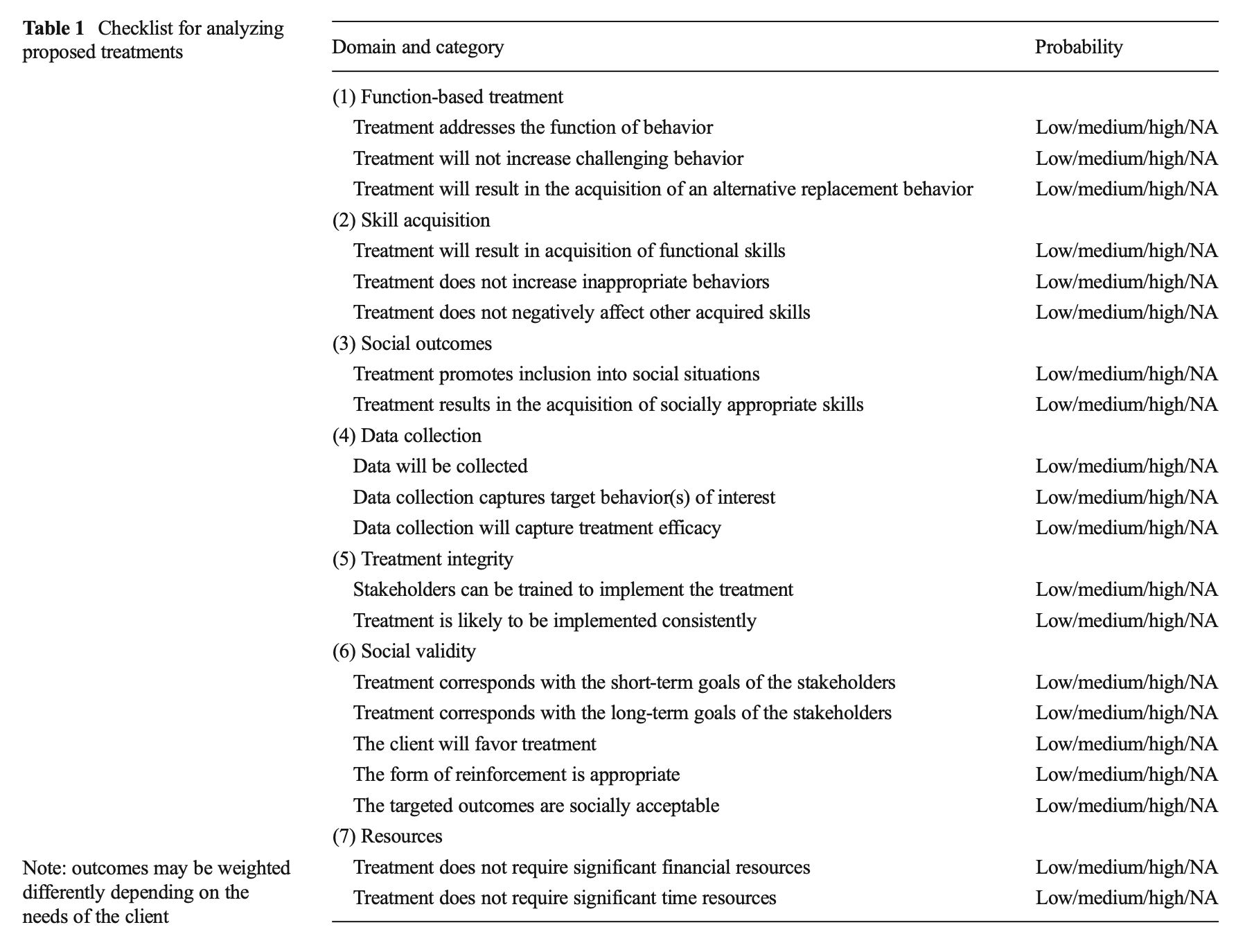
Brodhead's Checklist for Analyzing Proposed Treatments (CAPT):
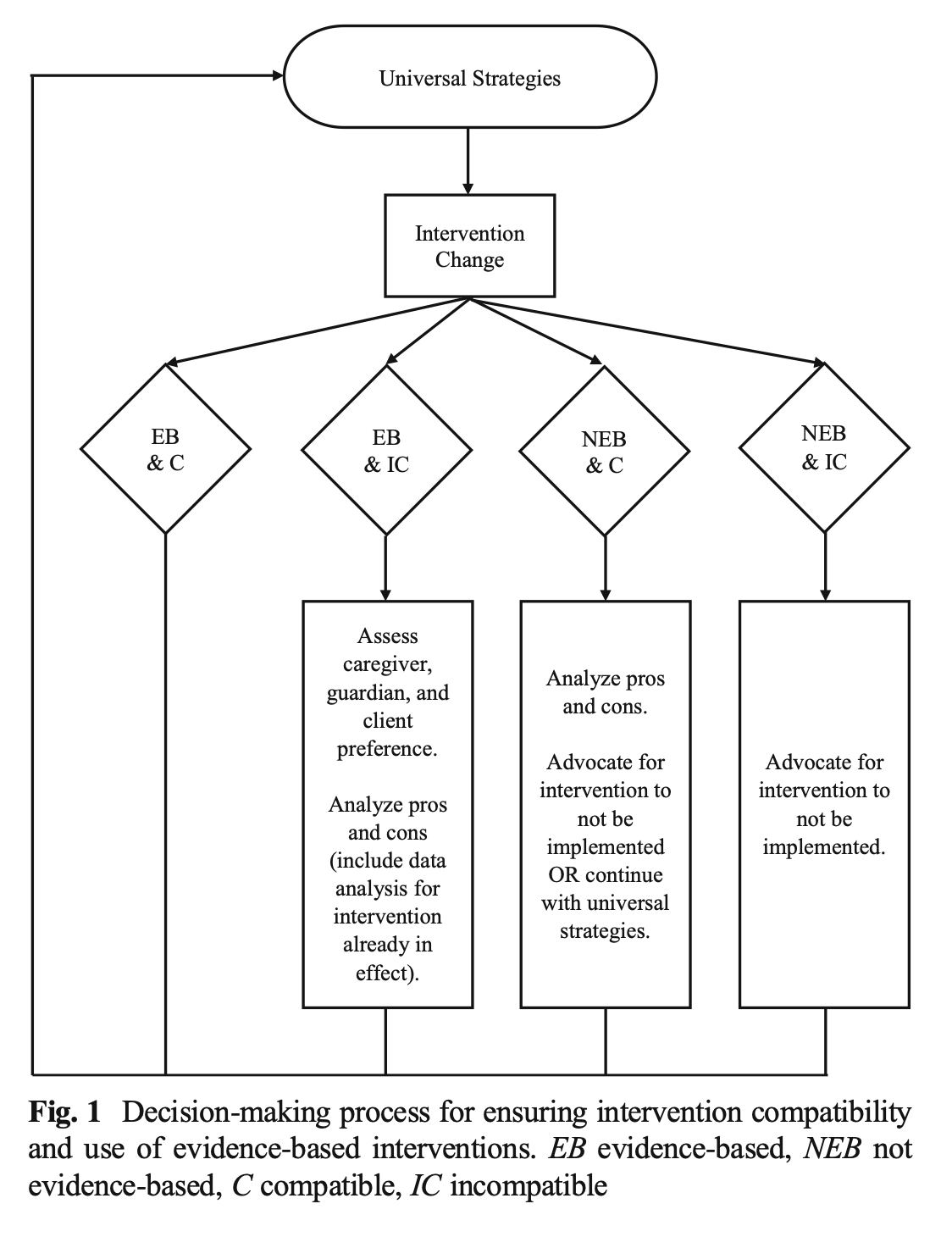
Newhouse-Oisten et al (2017) - Decision Making Process:
Brief List of Resources:
Foxx, Richard & Mulick, James. (2016). Controversial Therapies for Autism and Intellectual Disabilities.Routledge.ISBN: 978-1-138-80223-0
Montee BB, Miltenberger RG, Wittrock D, Watkins N, Rheinberger A, Stackhaus J. An experimental analysis of facilitated communication. J Appl Behav Anal. 1995 Summer;28(2):189-200. doi: 10.1901/jaba.1995.28-189. PMID: 7601804; PMCID: PMC1279809.
Navigating Non-behavioral Treatments:
- Matthew T. Brodhead (2015). Maintaining Professional Relationships in an Interdisciplinary Setting: Strategies for Navigating Nonbehavioral Treatment Recommendations for Individuals with Autism. Behav Analysis Practice 8:70–78. DOI 10.1007/s40617-015-0042-7
- Mindy K. Newhouse-Oisten, Kimberly M. Peck, Alissa A. Conway & Jessica E. Frieder (2017). Ethical Considerations for Interdisciplinary Collaboration with Prescribing Professionals. Behav Analysis Practice 10:145–153. DOI 10.1007/s40617-017-0184-x
-
Hawkins, R. P. (1974, March). Who decided “that” was the problem? Two stages of responsibility for applied behavior analysts. Paper presented at the Drake Conference on Professional Issues in Behavior Analysis, Des Moines, IA. https://files.eric.ed.gov/fulltext/ED092829.pdf
-
LaFrance, D. L., Weiss, M. J., Kazemi, E., Gerenser, J., & Dobres, J. (2019). Multidisciplinary teaming: Enhancing collaboration through increased understanding. Behavior Analysis in Practice, 12, 709-726
-
Lilienfeld, S., Marshall, J., Todd, J., & Shane, H. (2014). The persistence of fad interventions in the face of negative scientific evidence: Facilitated communication for autism as a case example. Evidence-Based Communication Assessment and Intervention, 8:2, 62-101. https://doi.org/10.1080/17489539.2014.976332
-
McGinnis, J. C. (in press). Introduction to primary care behavioral pediatrics: A guide for behavior analysts. Routledge.
-
Miliotis, A., & Weiss, M. J. (2021). Clinical corner: What are some ethical and practical considerations when collaborating with nonbehavioral service providers? Association for Science in Autism Treatment, 18. https://asatonline.org/research-treatment/clinical-corner/collaborating-with-nonbehavioral-service-providers
-
Walmsley, C., & Baker, J. C. (2019). Tactics to evaluate the evidence based of a nonbehavioral intervention in an expanded consumer area. Behavior Analysis in Practice, 12, 677–687.
Supplemental Resources:
Position Statements by Professional Organizations Related to FC:
- American Academy of Child and Adolescent Psychiatry. (1993, October). Policy statement of Facilitated Communication. AACAP Newsletter, February 1994. Reviewed June 2008.
- American Academy of Pediatrics. (1998). Auditory integration training and Facilitated Communication for autism. Pediatrics, 102, 431-433. This was reaffirmed in 2009.
- American Association on Mental Retardation. (1994). AAMR Board approves policy on Facilitated Communication. AAMR News & Notes, 7(1). Now called the American Association on Intellectual and Developmental Disabilities.
- American Association of Intellectual and Developmental Disabilities (2019) Facilitated Communication and Rapid Prompting Method: Position Statement of the AAIDD Board of Directors.
- American Psychological Association. (1994). Resolution on Facilitated Communication by the American Psychological Association. Adopted in Council, August 14, 1994, Los Angeles, California.
- American Speech-Language-Hearing Association. (2018). Facilitated communication [Position Statement]. www.asha.org/policy/
- Association for Behavior Analysis. (1995). Statement on Facilitated Communication. ABA Newsletter, 18,(2).
- International Society for Augmentative and Alternative Communication (2014). ISAAC Position Statement on Facilitated Communication, Augmentative and Alternative Communication, 30:4, 357-358, https://doi.org/10.3109/07434618.2014.971492
- Victorian Advocacy League for Individuals with Disability. Position Statement on the Use of Facilitated Communication.
Position Statements by Professional Organizations Related to RPM:
|


