Cost Benefit Analysis - Case Studies
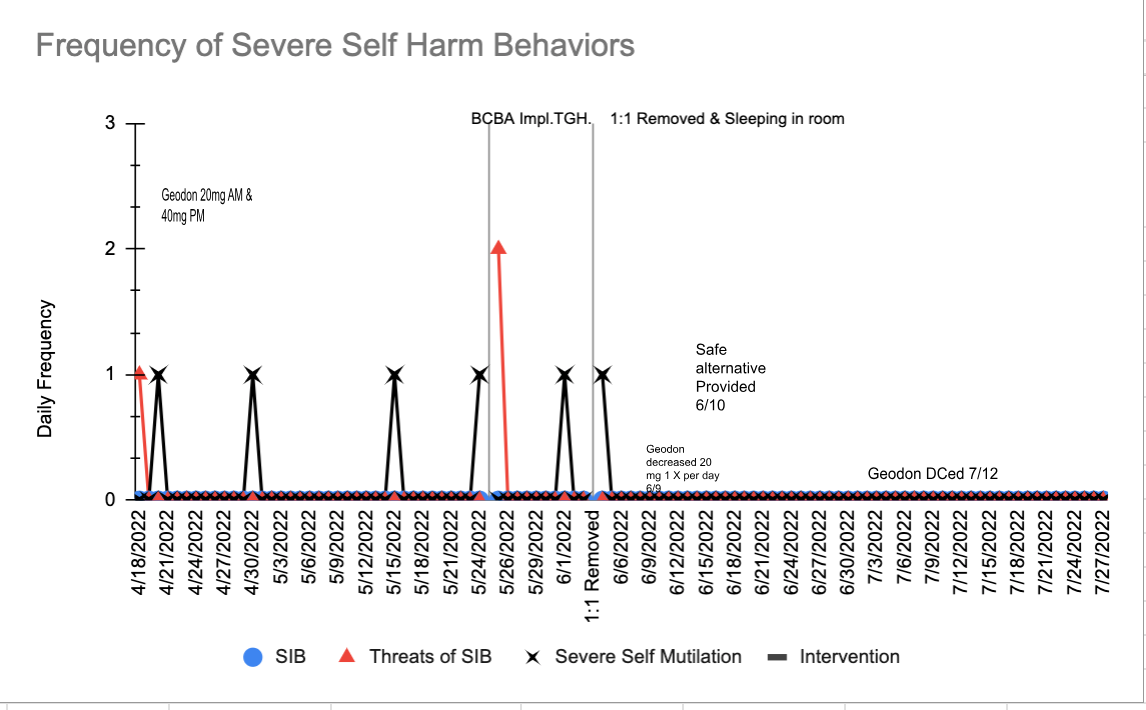
Case Study 1: Severe Self Mutilation
• Six incidents resulting in hospitalization over two months
• ~$19,000 per incident
• Baker Act placement in psychiatric hospital after each incident
• $2,000-$9,000 per stay ~$5,000 average
• Psychiatric Medication Discontinued:
• $144,000 total costs
• ABA individual service intervention - no hospital stays
• 86.5 hours over two weeks - $8650 cost of intervention
• For every $1 spent on ABA services $16 saved in hospitalization costs
The medication that this individual received due to problem behavior was also discontinued. Finally, this Cost Benefit Analysis is only based on hospitalization and Baker Act costs over this limited time period. Prior information on the number and costs of previous Baker Acts and other failed interventions for this individual were not available for this calculation.
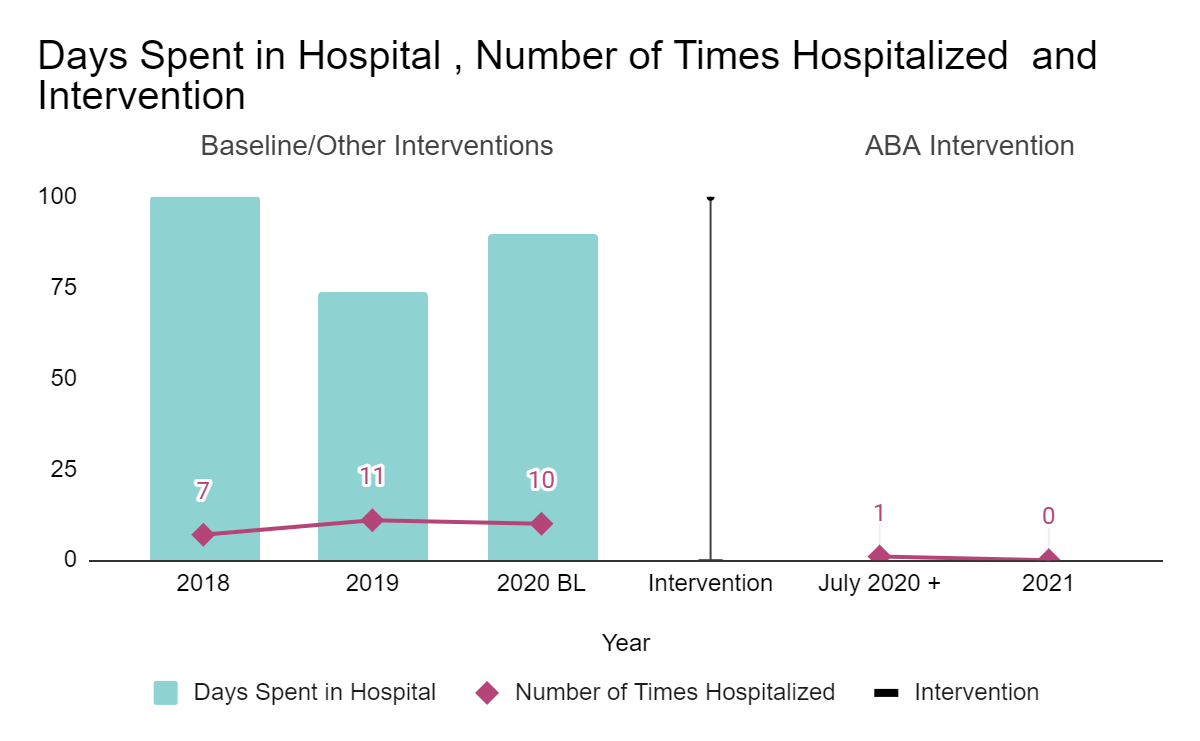
Case Study 2: Ingesting Dangerous Items
In this case study, specific hospitalization costs were not readily available. However, assuming similar costs over this 3 year period (~$19000 per hospital stay x 28 stays) the estimated costs would be $532,000.
Following ABA intervention by ATBx there was only 1 hospitalization for the second half of 2020 and no hospitalizations in 2021.
Estimated costs of hospitalizations in the first half of 2020 was already near $200,000 (10 incidents x ~$19000/incident). Assuming a similar number would have occurred the second half of 2020 this would have cost an additional $190,000. With only one incident for the rest of 2020 this would have saved an estimated $171,000. In 2021, assuming that if the intervention had not occurred we would have seen a similar pattern, this would have resulted in an additional $171,000 in hospital costs. Based on the cost of intervention in 2020-2021 and the cost savings associated with reductions in hospitalizations, for every $1 spent on ABA services almost $6 was saved in future hospital costs. In 2022 and 2023 there have also been no incidents. If we include these potential savings for every $1 spent on ABA services nearly $12 was saved in hospital costs. Additionally, medications were also discontinued for this individual, those costs as well as the costs of previously implemented failed interventions are not calculated into this analysis.
• 28 hospital stays over three years
• ~$532,000
• ABA - one incident
• 2021 savings ~$200,000
• For every $1 spent on ABA services almost $6 was saved in future hospital costs. In 2022 and 2023 there have also been no incidents. If we include these potential savings for every $1 spent on ABA services nearly $12 was saved in hospital costs.
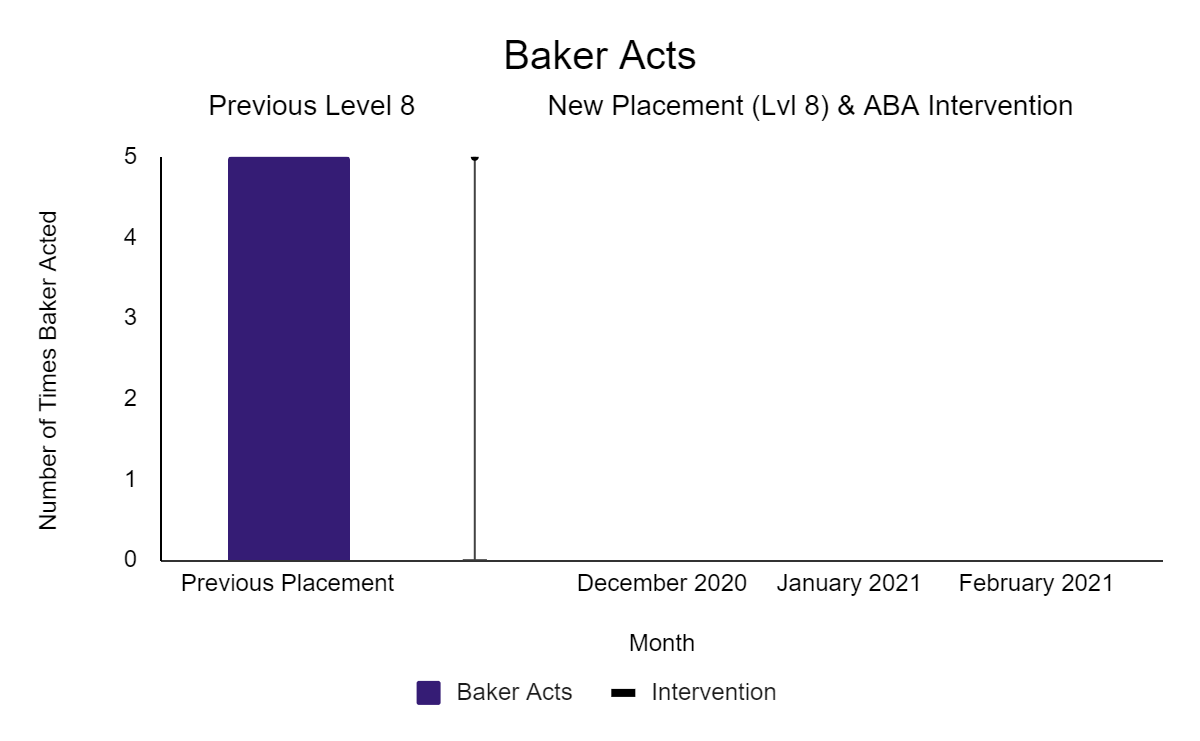
Case Study 3: Baker Acts
In this case study, Costs for Baker Act hospitalization were estimated as described above. Five incidents in previous placements in 2020 would cost ~ $25,000. Following the ATBx ABA intervention, there were zero Baker Act incidents across 3 months.
|